Dental Visits Overview

There are many dental procedures used to treat a variety of dental conditions. Knowing what to expect before, during, and after a procedure will help to make the experience go as smoothly as possible as well as aide in the recovery process. Here are the treatments that Michaels Dental offers its patients ranging from the most routine of checkups to the more complicated implant surgeries. Our job is to understand and help you while making your dental visit a comfortable one.
Visit our NEW PATIENT section to learn what a first time visit with Michaels Dental will include.
Replacing Missing Teeth

Missing teeth can be replaced in a variety of ways.
You may be a candidate for any one or all of them, depending on the circumstances. Implants are becoming the treatment of choice for a number of reasons. Most significant among these is the expected longevity, strength and stability offered by current implant treatment, as well as the predictability of implant treatment with current technologies. Listed below are common treatment options for missing teeth.
Options which do not come out of your mouth:
Implants

If you are a candidate for an implant, it is by far usually the most predictable and long-lasting replacement. The strength resembles your natural tooth and most people can eat the foods they used to eat. Implants are also the replacement which most closely duplicates your natural tooth. Implants are the only replacement which do not destroy any part of an existing tooth, or place undue stress on remaining teeth.
Throughout history, options for teeth replacement have changed and improved: from dentures, to partial dentures, to bridges, to implants. For those who are not candidates for implant therapy, these other options still exist.
An implant is also versatile. It can be used to replace one tooth, or multiple teeth. Implant bridges can be used to replace multiple teeth in a single area. Implants can be used to retain dentures by clicking or locking into the implant(s). Once the implant is in place, the top (abutment) of the implant can be changed to allow for changing options as the need arises. For example, if you have implants replacing one or multiple teeth, and eventually need a denture, the same implants can be modified and used to hold the denture. This is not possible with any other option for replacement.
Fixed Bridge

Teeth can also be replaced with a fixed bridge if there are teeth in the area that are adequate in number and sufficiently healthy and strong to support the artificial teeth. In order to fabricate a bridge, the adjacent teeth are prepared by reducing their size (or cut down) to remove all the enamel, making room for the prosthetic tooth restoration. A prosthetic tooth (or teeth) can be suspended between adjacent teeth in this way to provide a functional and cosmetic replacement for the missing tooth.
The limitation of this form of treatment has to do with the irreversible preparation of the adjacent (abutment) teeth for support. This exposes them to the risk of trauma to their nerves, raising the risk of requiring root canal treatment. Long-term, fixed bridges between natural teeth have an average life expectancy of 7-10 years before requiring replacement. Most bridges need replacement because people form cavities due to ineffective cleaning in such a difficult area, not because the bridge itself has any problems. Replacement of fixed bridges often entails further treatment as the abutment or supporting teeth have been further compromised over time by this advancing dental disease (such as cavities or periodontal bone loss).
Options which are removable: Dentures
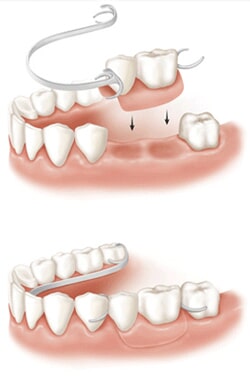
Removable partial or full dentures can replace a single missing tooth, several teeth, or all of the teeth in your upper and/or lower jaw. Dentures rely on support by the other teeth in that jaw (for partial dentures) and from mechanical support by the remaining ridge of gum and underlying bone. This support places stresses on remaining teeth which they are not meant to handle (partial dentures) or destroys the underlying bone (full dentures.) Without bone, retention and support are lost; this is why often the first denture is remembered as the best. And once this bone is lost, it is very difficult, if not impossible, to predictably regain what you once had. Maxillary (upper jaw) full dentures also may be helped by suction between the denture and the underlying gum of your palate (roof of mouth).
Dentures are usually about 6% as effective as your natural teeth. They are better than no teeth, but they are not a true replacement.
Why should I replace a tooth/teeth?
Reasons for replacing a missing tooth (or teeth) vary and should be weighed against the risks of leaving the space, as well as resultant changes that may take place in the rest of your dentition.
If you are missing a couple of teeth:
Drifting
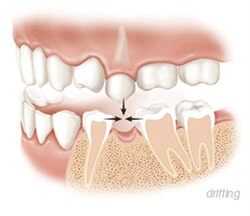
Loss of one or two teeth in a segment of your mouth can lead to drifting of neighboring teeth, whereby the adjacent teeth lean over into the vacant space where the teeth have been lost. Similarly, loss of a tooth or teeth can lead to shifting of opposing teeth as they drift down into the open space (super-erupt).
In general, our teeth have a constant tendency to move both towards the front of our mouths and towards the opposing jaw, unless they are stopped by something in their way, usually the adjacent or opposing teeth. Loss of teeth allows this to proceed in a pathologic way. As teeth drift, they create discrepancies in the height and contours of the gum tissue that predispose adjacent teeth to periodontal disease progression and/or dental decay from accumulation of food and plaque and difficulty in cleaning these areas from “piled-up” gum tissue. Drifting teeth can also adversely affect the occlusion (bite), as well as cosmetics of your face and smile.
If you are missing a few more teeth:
Collapse
People adapt, and many are able to function with missing, or even no teeth. This does not mean that this is healthy. It is a fact that as we age our digestive tract slows down, the muscles which move the food along the digestive tract do not function as well. At the same time, our glands do not produce as much lubricant to help with this process as they did in the past. Add to this that most people are on multiple medications which cause dryness mouth (xerostomia) and other mucous membranes which again retards the ability of the food to pass through the digestive tract. Now, because teeth are missing, our bodies are further challenged because food enters the digestive tract in bigger pieces which must be broken down and digested by an already compromised digestive system. It is obvious why people experience IBS (irritable bowel syndrome), GERD (Gastroesophageal reflux disease), etc. Replacing missing teeth is the first part of repairing this system, and the most predictable long-term way of reducing these problems.
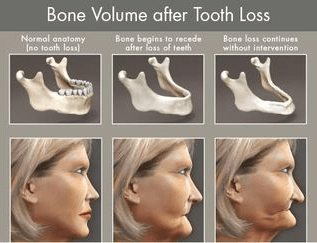
Why do I care about bone loss?

Without alveolar bone (bone which holds or held teeth), your denture is loose, your bridge catches food (which can lead to decay and replacement), and you may lose the option of choosing an implant as bone houses the implant.
When teeth are removed from the jaw, the bone that supports the teeth tends to shrink over time. This process is called resorption and is a natural consequence of the loss of stimulation to the bone from the forces placed on the teeth. This is similar to atrophy or shrinkage of muscles when they are no longer used. Resorption of the alveolar bone (bone that supports the teeth) begins almost as soon as the tooth is removed and proceeds over time. The bone will lose both height and width from resorption.
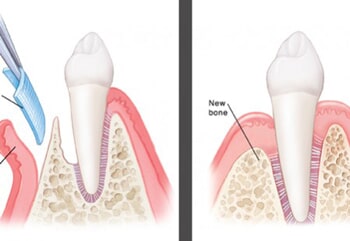
The easiest way to prevent bone loss is to prevent it. If a tooth is removed and a graft or implant is placed (image without preservation and with preservation), the bone retention is highest. The longer the problem goes, the harder it is to fix. If you want to lose five pounds, it is easier than if you want to lose 55 pounds.

When multiple teeth are lost, with or without a prosthesis to replace them, significant loss of jawbone can take place. This sometimes leads to difficulty wearing a removable denture due to lack of an adequate “ridge” upon which the denture can obtain stability. In the so-called “esthetic zone” of the mouth, where loss of ridge volume can be visibly apparent to the naked eye, this can lead to a cosmetic defect. As the bone resorbs, the gum which covers it also shrinks away, creating a concavity (depression in height and width) that can be unsightly as well as possibly promote food impaction under adjacent teeth.
Maxillofacial Surgery

When facial reconstruction, including procedures involving the oral cavity, is called for, a specialist is needed.
Common maxillofacial procedures include denture-related procedures and jaw surgery.
Denture Fatigue
People who have worn dentures for a long time often experience loss of gum tissue and even bone, mostly from the wear and tear of the appliance on the soft tissues of their mouth.
In some cases, maxillofacial surgery, including bone grafts, manipulation of soft tissues or even jaw realignment, may be performed to correct such problems.
Jaw Correction
Protruding chins, crooked or buck teeth or misaligned teeth are good candidates for maxillofacial surgery.
In some people, jaws do not grow at the same rate; one may come in larger than the other, or simply not be aligned properly with other bony structures in the skull. This can cause problems other than appearance issues; an improperly aligned jaw can cause problems with the tongue and lips, and speech and chewing problems as well. Jaw surgery can move jaws into their proper place.
Other kinds of maxillofacial surgery can correct problems with upper facial features such as the nose and cheek.
In addition to correcting jaw problems surgically, orthodontic appliances such as braces may be needed to restore bite relationship and ensure continued proper alignment of the jaw. In some cases, tiny wires or small rubber bands may be needed to keep the jaws in place and promote faster healing. In other cases, small “fixation” screws or plates may need to be inserted in the jaws to facilitate easy movement of the jaws following surgery.
Crowns

Crowns fit over a tooth, like a hat (or cap) fits on your head, to reinforce a weakened tooth. A crown is usually made of a material like porcelain and cemented into place.
Crowns are typically used to restore a tooth’s function and appearance following root canals or cuspal fractures, or to prevent further fracture of a weakened tooth. When decay in a tooth has become so advanced that large portions of the tooth must be removed, crowns are often required to restore the tooth.
Crowns are also used to attach bridges, cover implants, prevent a cracked tooth from becoming worse, or reinforce an existing filling is in jeopardy of becoming loose or dislocated. Crowns also serve an aesthetic use and are applied when a discolored or stained tooth needs to be restored to its natural appearance.
Procedures
A tooth must usually be reduced in size to accommodate a crown. An impression is made of the existing tooth and a cast is made. The impression is sent to a special lab, which manufactures a custom-designed crown. In some cases, a temporary crown is applied until the permanent crown is ready. Permanent crowns are cemented in place.
Crowns are sometimes confused with veneers, but they are quite different. Veneers are typically applied only to relatively small areas.
Caring for Your Crowns
With proper care, a good quality crown could last 7-10 years or longer. The longevity of your crown can depend on the quality of your dentist, the lab used and your care, as well as the state of the tooth before it was crowned. Just like bridges, it is rare that the crown itself breaks down; it is most often a cavity that develops farther down on the tooth due to difficulties in cleaning the area or recession exposing the weaker root surface to cavity-forming bacteria. It is very important to clean the area around the crown to avoid excess plaque or collection of debris around the restoration.
Certain behaviors such as jaw clenching or bruxism (teeth grinding) significantly shorten the life of a crown. Moreover, eating brittle foods, ice or hard candy can compromise the adhesion of the crown, or even damage the crown.
Dentures

A denture is a removable option for missing teeth and adjacent tissues. It is made of acrylic resin, sometimes in combination with various metals. A denture is a prosthesis for teeth similar to a prosthetic arm or leg. Some people adjust easily to dentures, and some people never adjust.
Types of Dentures
Complete dentures include all the teeth, while a partial denture fills in the spaces created by missing teeth and utilizes the remaining teeth to distribute forces previously carried by missing teeth.
Candidates for complete dentures have lost most or all of their teeth. A partial denture is suitable for those who have some healthy, natural teeth remaining. A denture improves chewing ability and speech and provides support for facial muscles. It will greatly enhance the facial appearance and smile.
Complete or full dentures are made when all of your natural teeth are missing. You can have a full denture on your upper or lower jaw, or both.
Complete dentures are called “conventional” or “immediate” according to when they are made and when they are inserted into the mouth. Immediate dentures are inserted immediately after the removal of the remaining teeth. To make this possible, the dentist takes measurements and makes the models of the patient’s jaws during a preliminary visit.
An advantage of immediate dentures is that the wearer does not have to be without teeth during the healing period. However, bones and gums can shrink over time, especially during the period of healing in the first six months after the removal of teeth. When gums shrink, immediate dentures will require rebasing or relining to fit properly. A conventional denture can then be made once the tissues have healed. Healing may take at least 6-8 months.
An overdenture is a removable denture that fits over a small number of remaining natural teeth or implants. The natural teeth must be prepared to provide stability and support for the denture. Implants provide the support for the denture. Most people are able to eat what they want with over dentures. The support from the implants or natural teeth also minimizes the destructive forces of a conventional denture or partial.
Partial dentures are often a solution when several teeth are missing.

Removable partial dentures usually consist of replacement teeth attached to pink or gum-colored plastic bases, which are connected by metal framework. Removable partial dentures attach to your natural teeth with metal clasps or devices called precision attachments. Precision attachments are generally more esthetic than metal clasps and are nearly invisible. Crowns on your natural teeth may improve the fit of a removable partial denture and they are usually required with attachments. Dentures with precision attachments generally cost more than those with metal clasps. Implants with a partial denture helps distribute the forces and can increase the lifetime of the natural teeth remaining. Implants also reduce the need for visible clasps.
How Are Dentures Made?
The denture process takes about 4-6 weeks and five appointments: the initial diagnosis is made; an impression and a wax bite are made to determine vertical dimensions and proper jaw position; a “try-in” is placed to assure proper color, shape and fit; and the patient’s final denture is placed, following any minor adjustments.
First, an impression of your jaw is made using special materials. In addition, measurements are made to show how your jaws relate to one another and how much space is between them (bite relationship). The color or shade of your natural teeth will also be determined. The impression, bite and shade are given to the dental laboratory so a denture can be custom-made for your mouth.
The dental laboratory makes a mold or model of your jaw, places the teeth in a wax base, and carves the wax to the exact form wanted in the finished denture. Usually a “wax try-in” of the denture will be done at the dentist’s office so any adjustments you desire can be done before the denture is completed. Sometimes a second try-in appointment is scheduled to make sure your smile is the best it can be before permanently processing the denture. (This is not possible with an immediate denture.)
The denture is completed at the dental laboratory using the “lost wax” technique. A mold of the wax-up denture is made, the wax is removed and the remaining space is filled with pink plastic in dough form. The mold is then heated to harden the plastic. The denture is then polished and ready for wear.
Duplicate Dentures (Back-up Dentures)
At the time your permanent dentures are made, it is fairly easy for a second set of “back-up” dentures to be made. It is also less costly. Some patients opt to have this second set to use during relines, fabrication of new dentures, or if you accidentally break or lose your denture.
Getting Used to Your Denture
Unfortunately, no denture or partial denture replaces your missing teeth as they were. They fill space and allow you to adjust to a different way of speaking, eating and functioning. Overdentures usually yield the best result.
For the first few weeks, a new denture may feel awkward or bulky. However, for the majority of denture wearers, your mouth will eventually become accustomed to wearing it. Inserting and removing the denture will require some practice. Your denture should easily fit into place. Never force the partial denture into position by biting down. This could bend or break the clasps.
At first, you may be asked to wear your denture all the time. Although this may be temporarily uncomfortable, it is the quickest way to identify those denture parts that may need adjustment. If the denture puts too much pressure on a particular area, that spot will become sore. Your denture can be adjusted to fit more comfortably. After making adjustments, you will need to take the denture out of your mouth before going to bed and replace it in the morning. Start out by eating soft foods that are cut into small pieces. Chew on both sides of the mouth to keep even pressure on the denture. Avoid sticky or hard foods, including gum. You may want to avoid chewing gum while you adjust to the denture.
Care of Your Denture
It’s best to stand over a folded towel or a sink of water when handling your denture, just in case you accidentally drop it. It is less likely to break if it lands on a towel. Brush the denture (preferably with a denture brush) daily to remove food deposits and plaque, and keep it from becoming permanently stained. Avoid using a brush with hard bristles or toothpaste, which can damage the denture. Look for denture cleansers with the American Dental Association (ADA) Seal of Acceptance. Pay special attention to cleaning teeth that fit under the denture’s metal clasps. Plaque that becomes trapped under the clasps will increase the risk of tooth decay. This is the most common cause of loss of these teeth.
Hand soap or mild dishwashing liquid to clean dentures is also acceptable. Other types of household cleaners and many toothpastes are too abrasive and should not be used for cleaning dentures. A denture could lose its proper shape if it is not kept moist. At night, the denture should be placed in soaking solution or water. However, if the appliance has metal attachments, they could be tarnished if placed in soaking solution. Not removing your denture at night leads to accelerated bone loss (leading to dentures which fall out) and fungal infections under your denture and in your mouth.
Even with full dentures, you still need to take good care of your mouth. Every morning, brush your gums, tongue and palate with a soft-bristled brush before you put in your dentures. This removes plaque and stimulates circulation in the mouth. Selecting a balanced diet for proper nutrition is also important for maintaining a healthy mouth.
Your denture will need to be relined every 3-5 years. Because the supporting bone and gums under the denture changes in this amount of time, the denture will start to “loosen” or become ill-fitting. A new denture is usually made at around 10 years, or when the teeth wear out. Gaining or losing weight will also affect the fit of your denture; it may need to be relined if you lose a significant amount of weight.
Even with dentures, you should maintain annual checkups with your dentist. At this time, the fit of the denture will be evaluated, and your dentist can check for any signs of oral cancer. It is lifesaving to catch oral cancer early!
Adjustments
Over time, adjusting the denture may be necessary. As you age, your mouth naturally changes, which can affect the fit of the denture. Your bone and gum ridges can recede or shrink, resulting in a loose-fitting denture. Loose dentures can cause various problems, including sores or infections. Dentures that do not fit properly can be adjusted. Avoid using a do-it-yourself kit to adjust your dentures, as this can damage the appliance beyond repair. Glues sold over the counter often contain harmful chemicals and should not be used on a denture. These glues also leave a residue preventing strong bonding for repairs or tooth replacement.
If your denture no longer fits properly, if it breaks, cracks or chips, or if one of the teeth becomes loose, see your dentist immediately. In many cases, dentists can make necessary adjustments or repairs, often on the same day. Complicated repairs may require that the denture be sent to a special dental laboratory.
Over time, dentures will need to be relined, re-based, or re-made due to normal wear. To reline or re-base a denture, the dentist uses the existing denture teeth and refits the denture base or makes a new denture base. Dentures may need to be replaced if they become loose and the teeth show signs of significant wear.
Common Concerns
Eating will take a little practice. Start with soft foods cut into small pieces. Chew slowly using both sides of your mouth at the same time to prevent the dentures from tipping. As you become accustomed to chewing, add other foods until you return to your normal diet.
Continue to chew food using both sides of the mouth at the same time. Be cautious with hot or hard foods and sharp-edged bones or shells.
Some people worry about how dentures will affect their speech. Consider how your speech is affected when you have a number of your natural teeth missing. Most people adjust quickly.
Pronouncing certain words may require practice. Reading out loud and repeating troublesome words will help. If your dentures “click” while you’re talking, speak more slowly. You may find that your dentures occasionally slip when you laugh, cough or smile. Reposition the dentures by gently biting down and swallowing. If a speaking problem persists, consult your dentist.
You will notice excess salivation at first. This is because your mouth believes the denture is food and tries to digest it. This will stop as your mouth adjusts to the denture.
Denture Adhesives
Denture adhesives can provide additional retention for well-fitting dentures. Denture adhesives are not the solution for old, ill-fitting dentures. A poorly fitting denture, which causes constant irritation over a long period, may contribute to the development of sores. These dentures may need a reline or need to be replaced. If your dentures begin to feel loose, or cause pronounced discomfort, consult with your dentist immediately.
Flap Surgery
Your bone and gum tissue should fit snugly around your teeth like a turtleneck. When you have periodontal disease, this supporting tissue and bone is destroyed, forming “pockets” around the teeth. Over time, these pockets become deeper, providing a larger space for bacteria to thrive and wreak havoc.
As bacteria accumulate (called tartar, or calculus) and advance under the gum tissue in these deep pockets, additional bone and tissue loss follow. Eventually, if too much bone is lost, the teeth become mobile because there is no bone remaining to hold them in place. This is periodontal disease and if it continues, teeth will be lost as well as supporting bone. (See “Why do I care about bone loss?”).
Flap surgery is sometimes performed to remove tartar deposits in deep pockets or to reduce the periodontal pocket and make it easier for you, your dentist, and your hygienist to keep the area clean. This common surgery involves reflecting the gum tissue and removing the tartar. The gums are then gently replaced so that the tissue fits snugly around the tooth again.
A pocket reduction procedure is recommended if daily at-home oral hygiene and a professional care routine cannot effectively reach these deep pockets.
In some cases, irregular surfaces of the damaged bone are smoothed to limit areas where disease-causing bacteria can hide. This allows the gum tissue to better reattach to healthy bone. In other cases, additional bone may be placed, or grafted, to prevent further infection by bacteria, and give the teeth back some support.
Complex Tooth Removal

General Procedure
When restoration procedures such as root canal therapy, crowns, or fillings are not enough to save a tooth, it may need to be pulled, or removed, to prevent breakdown of other teeth or serious infections.
Tooth removal procedures today are close to painless, thanks to powerful anesthetics and sedatives. In almost all, a patient who has tooth pulled experiences little or no discomfort, and only minor bleeding.
Before a tooth is removed, the area surrounding the tooth is numbed with a topical/and or injectable anesthetic such as Lidocaine or Septocaine (Though many people are familiar with the word Novocaine, it has not been used for many years.).
It is important to consider bone grafting at the time of tooth removal if the tooth may ever be replaced. At the moment of tooth removal, you start to lose bone. The body believes this bone is no longer necessary since there is no longer a tooth to support. Socket or ridge preservation grafting can save time, future surgeries and loss of support which cannot usually be fully regenerated.
Patients with extracted teeth sometimes need to take an antibiotic, and at the very least, take precautions following the procedure to ensure that infection doesn’t occur.
Smoking, vigorous brushing and rinsing, and drinking liquids through straws are discouraged during the post-operative period because they hinder healing and may cause the wound to open. This is called Acute Alveolar Osteitis, or “dry socket” and can be more painful than any toothache itself. Cold compresses applied to the outside cheek near the extraction area can help reduce any swelling and promote faster healing.
Wisdom Teeth
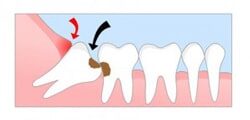
Wisdom teeth are the third and final set of molars that erupt in the back corners of the upper and lower normal adult mouth. Unfortunately, most people experience problems from wisdom teeth such as cavities on adjacent teeth when they erupt at an angle, improper bites, cyst formation and other, sometimes life threatening, problems (Ludwig’s Angina).
If wisdom teeth are not removed, they can sometimes become infected. Infected wisdom teeth can be extremely painful, as well as harmful to your oral health. Symptoms are easy to spot severe discomfort, inflammation, and some kinds of infections.
The bottom line is many people need to have their wisdom teeth removed to avoid future serious problems. These problems may not occur until a patient is in his/her 50’s 60’s or 70’s. At those ages removal is riskier and more difficult. To avoid these risks, most wisdom teeth are removed during the teen years or 20’s. In general, the lack of the four wisdom teeth does not hamper one’s ability to properly bite down, speak or eat.
If you experience any of the following symptoms, you may have an infected wisdom tooth:
- Facial swelling
- Infection
- Pain
- Gum swelling
Dr. Michaels has removed thousands of teeth and is able to remove most wisdom teeth for our patients. For the situations in which IV Sedation would work better for the patient, Dr. Michaels also offers this comfort for her patients.
Bridges

Bridges are natural-looking dental appliances that can replace a section of missing teeth. Because they are custom-made, bridges are barely noticeable and can restore the natural contour of teeth as well as the proper bite relationship between upper and lower teeth.
Bridges are sometimes referred to as fixed partial dentures, because they are semi-permanent and are bonded to existing teeth or implants. Some bridges are removable and can be cleaned by the wearer; others need to be removed by a dentist.
Porcelain, gold alloys or combinations of materials are usually used to make bridge appliances.
Appliances called implant bridges are attached to an area below the gum tissue, or the bone. These are wonderful because you can replace more teeth with fewer implants! For example, you can replace three teeth using only two implants.
If implants are not an option for you, a bridge is the best alternative. Though bridges require trimming the teeth next to the missing teeth, they are the only other replacement for your teeth which can be cemented in your mouth permanently.
Sealants

The pits and grooves of your teeth are prime areas for opportunistic decay. Even the best brushing sometimes misses some of these intricate structures on the chewing surfaces of your teeth.
Enter sealants, which are thin coatings applied to the chewing surfaces designed to prevent the intrusion of bacteria and other debris into the deep crevices on the tops of your teeth.
Sealants actually were developed about 50 years ago but didn’t become commonly used until the 1970s. Today, sealants are widely popular and effective. Senior adults are great candidates for sealants because of the difficult areas to reach, and the amount of dental work around which a patients must clean. Sealants can help to fill the nooks and crannies. Many times, a person’s dexterity diminishes so normal cleaning at home as not as effective as it was in the past. Sealants can sometimes be used to increase the longevity of an existing filling, or restoration, by sealing the area between the filling and the tooth. Young children are candidates for preventative measures like sealants because in many cases, decay has not set in. Even on teeth where decay is present, sealants have been shown to fight additional damage.
Sealants are applied by first cleaning the tooth surface. The procedure is followed by “etching” the tooth with an abrasive substance, which allows the sealant to better adhere. After the sealant is applied, a warm light source is directed to the site to promote faster drying. Sealants usually need re-application every 5 – 10 years and may need touch-ups in between.
Scaling and Root Planing
If you have a healthy mouth, or even if you have gingivitis, scaling and root planning (SRP) is not necessary. Small deposits of calculus and tartar can also be easily removed with a normal cleaning. This is when your hygienist uses hand instruments combined with an ultrasonic cleaner to most effectively remove bacteria which has hardened on your teeth.
If you have periodontal disease (any bone loss due to bacteria), it is impossible to clean these areas with home care or a regular cleaning; the bacteria has invaded deeper than can be normally cleaned, and it has started to dissolve the very bone which supports your teeth. To prevent this from progressing until there is no bone, and teeth are lost, a deeper cleaning is performed.
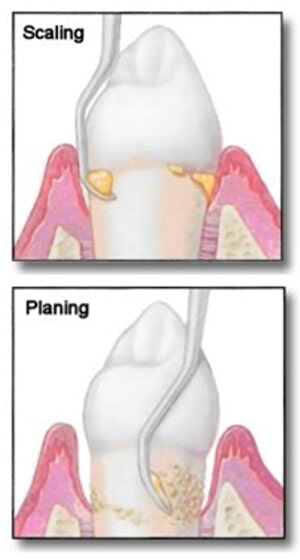
The procedure usually begins with administration of a local anesthetic to reduce any discomfort. The process is similar to pulling asphalt and debris out of a wound after a fall. It must be done, but it is best if it is numb. Then, a small instrument called a “scaler,” or an ultrasonic cleaner, is used to clean beneath your gum line to remove plaque and tartar. The ultrasonic waves clean in areas where our hand instruments could never reach.
The root surfaces on the tooth are then planed and smoothed. This lets the gum tissue heal and reattach itself to the tooth.
Fillings

What’s in a Filling?
Fillings, known clinically as amalgams, are synthetic materials that are used to restore a portion of a tooth damaged by decay or traumatic injury. There are different types of materials used to fill cavities, including resin, gold and metal alloys.
Conventional amalgams are the silver-colored material many people have had placed in their teeth following treatment of a cavity. Many amalgams are actually a combination of various metal alloys, including copper, tin, silver and mercury. Mercury, a binding agent used in amalgams, has come under scrutiny lately by some health officials who claim it may cause long-term health problems.
Is Mercury in a Dental Filling Safe?
The American Dental Association cautions that emotional reports claiming amalgam is responsible for a variety of diseases are confusing and perhaps even alarming people to the point where they will not seek necessary dental care. Moreover, the ADA maintains that there has been no scientific evidence to show that amalgams are harmful because the miniscule amounts of mercury are so stable, they present no risks to humans. There have been rare cases of patients developing allergic reactions to amalgams.
Amalgam is no longer used by Dr. Michaels.
Alternative Materials
There are alternatives to conventional substances used in amalgams, such as gold and metal alloys. These include materials made from porcelain and composite resins, which are colored to match natural tooth enamel.
Common amalgam alternatives include:
- Composite fillings – As stated, composite fillings are just what the name implies: a mixture of resins and fine particles designed to mimic the color of natural teeth. Dr. Michaels uses a sonic filling device which assures the best possible adaptation of the filling material to your tooth. This technology provides the best seal for your tooth minimizing the bacteria from accumulating and causing more cavities.
- Ionomers – Like composite resins, these materials are tooth-colored. Ionomers are made from a combination of various materials, including ground glass and acrylic resins. Ionomers are typically used for fillings near the gum line or tooth root, where biting pressure is not a factor. They are more fragile than other fillings, however, the material itself gathers and retains fluoride to help strengthen the tooth. Sometimes Dr. Michaels will prescribe a high fluoride tooth paste to be absorbed by the fillings and enhance the tooth’s resistance to recurrent cavities.
- Porcelain (ceramic) – These materials are usually a combination of porcelain, glass powder, and ceramic. Candidates for porcelain fillings are typically crowns, veneers, and onlays and inlays. Unlike ionomers, porcelain fillings are more durable, but can become fractured if exposed to prolonged biting pressures. There is also evidence to suggest that onlay, and/or inlays can cause fracturing of teeth. Dr. Michaels uses these material for crowns and veneers. In these situations, they provide a durable, long-lasting restoration.
Jaw / TMJ
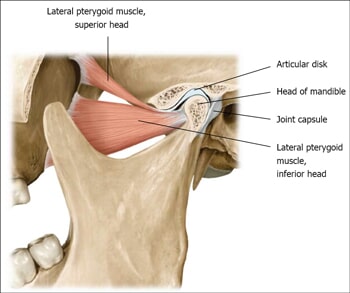
People who grind their teeth can sometimes develop a serious problem with their jaw, which left untreated, can adversely affect the teeth, gums and bone structures of the mouth.
One of the most common jaw disorders is related to a problem with the temporomandibular joint, the joint that connects your lower jaw to your skull and allows your upper and lower jaw to open and close and facilitates chewing and speaking.
People with temporomandibular joint disorders (TMD) often have a clicking or popping sound when opening and closing their mouths. Such disorders are often accompanied by frequent headaches, neck aches, and in some cases, tooth sensitivity.
Some treatments for TMD include muscle relaxants, aspirin, biofeedback, or wearing a small plastic appliance in the mouth during sleep.
Minor cases of TMD involve discomfort or pain in the jaw muscles. More serious conditions involve improperly aligned joints or dislocated jaws. The most extreme form of TMD involves an arthritic condition of the jaw joint. Traumatic injuries also can cause jaw dislocation.
In these cases, jaw surgery, may be required to correct the condition. Some jaw surgery can be performed arthroscopically.
